In the previous part I had told you how to identify if you are a potential candidate for developing Glaucoma, the Silent Thief of sight. Now it is time to look at the different ways you can confirm if you have the disease.
Detecting glaucoma, in most instances, does not require sophisticated equipment. Ophthalmologists can identify features of the disease by just using some common instruments that they already possess. If a systematic approach is done the disease can be picked up early.
1. SLIT LAMP EXAMINATION

During preliminary examination with the instrument called the slit lamp the ophthalmologist may see some features that point to the presence of glaucoma. There maybe shallowing of the anterior chamber, the space between the cornea and the iris suggesting a possibility of angle closure glaucoma. There can be pigments on the inner surface of the cornea, or some flaky white material on the surface of the lens called pseudo-exfoliation.
2. TONOMETRY
The next step will be to see if your intraocular pressure (IOP) is raised. Remember though, glaucoma needn’t always be associated with an elevated IOP. There are eyes that have glaucoma even with normal or low pressures. IOP, therefore, is not the main criteria for deciding if you have glaucoma. IOP is measured by an instrument called the applanation tonometer, attached to the slit lamp. After instilling a drop of anesthetic the tip of the instrument is made to touch the dome of your cornea and a reading is taken from a rotating dial on the side of the instrument. There are other instruments to measure the IOP but the applanation tonometer is take as standard.

3.PACHYMETRY
Sometimes the IOP maybe normal or below normal but other features may give an indication that the eye has been affected significantly by glaucoma. The ophthalmologist may then do a pachymetry, a test done to measure the thickness of the cornea.
It is not unusual to have people with myopia (short sightedness) to have a thin walled eye. This gives a falsely low reading of IOP. The reverse maybe true in other eyes. Due to a thicker cornea, the recorded IOP might by high, but there may not be any evidence to suggest glaucoma. Such eyes with higher IOP but without features of glaucoma are designated as Ocular Hypertension, and will need follow up to see if they progress to glaucoma.
4. OPTIC NERVE HEAD EVALUATION
After having measured the IOP the next step is to look inside your eye to see if there is any physical damage to your optic nerve head (ONH). This is the most important part of the examination that lets the ophthalmologist decide if your eye has been affected by glaucoma and if you need any treatment. The ONH can be examined by a simple hand held instrument called the ophthalmoscope; a self illuminating, hand held instrument that is held close to your eye and the doctor looks inside from the other side.

For greater details, a small, powerful hand held lens (a 78 or 90 diopter) is used in combination with the slit lamp bio-microscope. It gives a bigger 3D view of the ONH and any damage can be assessed easily.

This is the most important step in the assessment of a person suspected to have glaucoma. Features onthe ONH or surrounding retina can instantly clinch the diagnosis of glaucoma. The doctor will look for certain changes in the ONH that will show if glaucoma has already damaged the eye. I will dwell a little longer on this part of the exemination because, of all the examinations, this is the single most critical test that gives the doctor a hint that you have glaucoma.
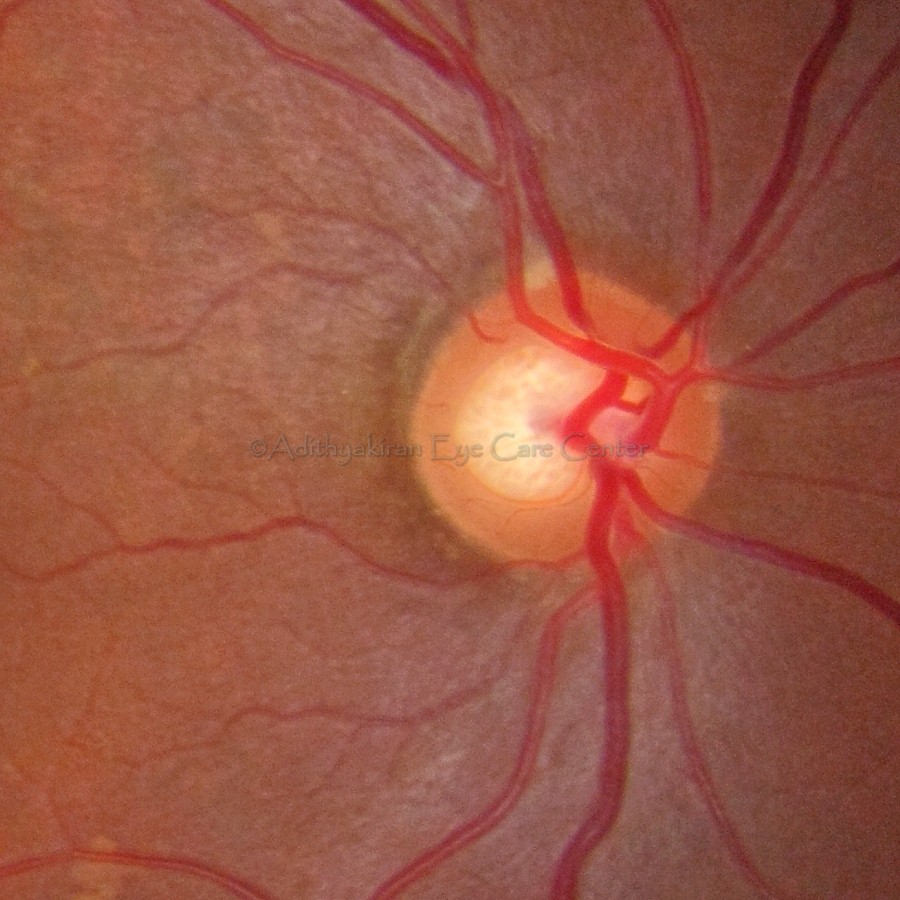
To know what features suggest damage to the doctor, you should know what a normal ONH looks like. The optic nerve is the bundle of nerve fibres that start from your retina and go towards the visual cortex of your brain. As they exit the eye they form a distinct round or slightly oval disc, orange in colour, called the optic disc (see figure above). In the center of the disc (blue circle in figure below) is a smaller, light yellow coloured portion called the optic cup (yellow circle in figure below). This cup is usually well centered or slightly eccentric, when surrounded by heathly nerve fibers.

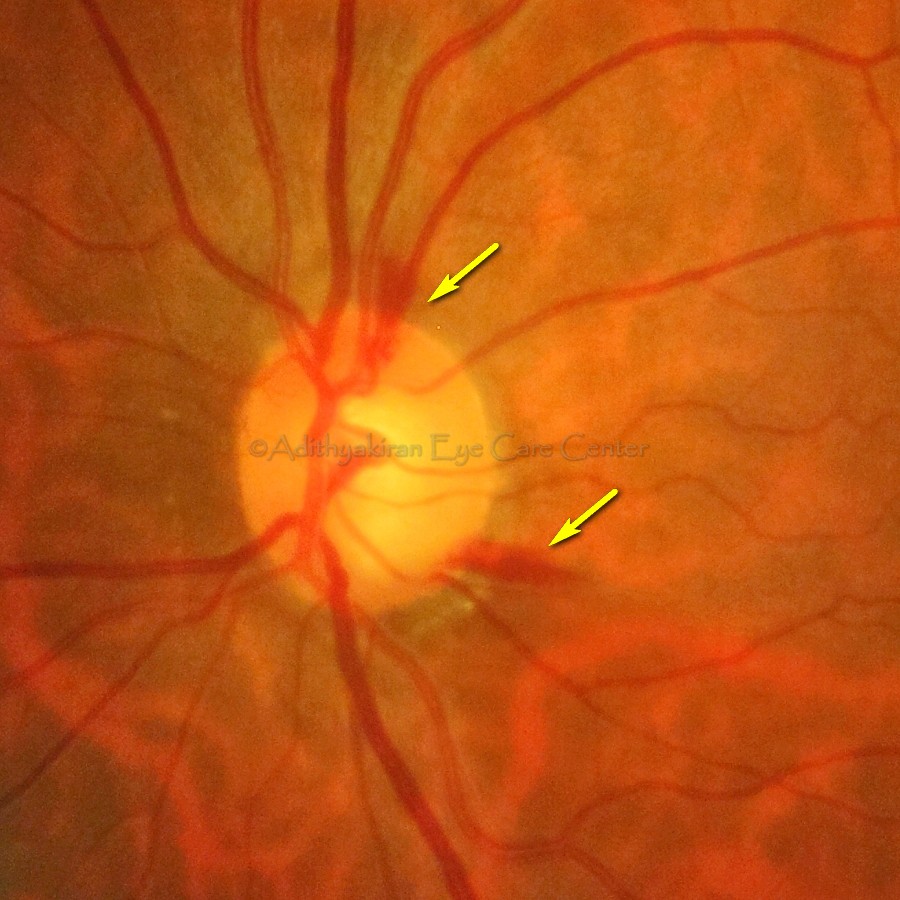
The portion between the blue and yellow ring represents healthy nerve fibers and they are present in all quadrants of the disc in slightly varying widths. This part is called the neuro-retinal rim (NRR). The first sign of damage is a narrowing of the NRR, (red arrow) sometimes all the way upto the edge of the disc.

Sometimes associated with this narrowed rim there can be other signs that indicate the presence of active glaucoma. There might be small hemorrhages (bleeding) along the disc margin (yellow arrows in the picture below).
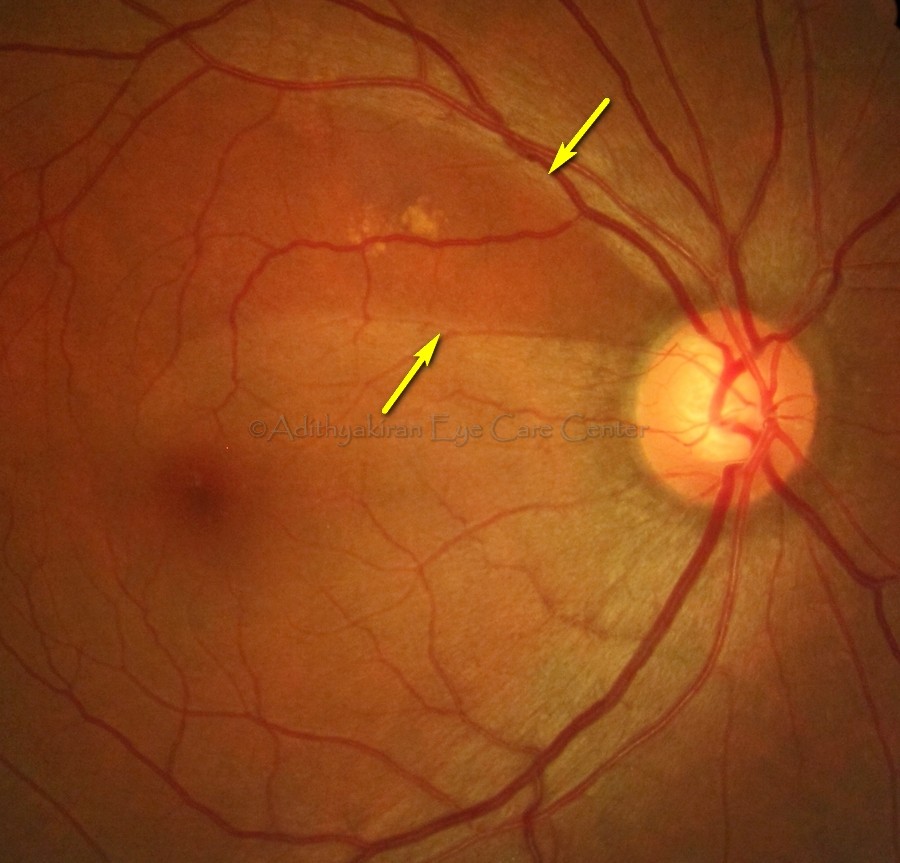
In some eyes, there is a dark band on the retina corresponding to the area of narrowing of NRR (between yellow arrows in the picture below). They are areas of retinal thinning due to loss of some tissue there. They are called retinal nerve fiber layer (RNFL) defects. They usually correspond to defects in the visual field tests.
You can see that an ophthalmologist can make an instantaneous diagnosis of glaucoma if any of the above mentioned findings are there in a patient’s eye. Very simple instruments and equipment are need to make a diagnosis. It is only in cases where the findings are borderline that we need sophisticated instruments to give additional information to support the diagnosis.
Once glaucoma is detected the next step is to assess how much damage it has done to the eye. Damage to visual function usually occurs from the periphery of your vision. This is assessed by a test that plots the visual field. More about that in the next post.
