As usual this interjection is because of a patient who walked in just now. She is a spectacle wearer since the age of 5. She has been having little annoying dots in front of her eyes that she couldn’t get rid off. I was querying her about her history of using spectacles and the conversation went something like this.
Me: When did you get your spectacles last?
She: A year ago.
Me: Where did you get your eyes checked then?
She: At the optical shop. (I’m not mentioning the name since it is close to my clinic).
Me: Who checked your eye there?
She: There was a doctor there.
Me: Were you dilated and examined.
She: No. They tested me on a computer.
Me: Then where did you get your glasses prescribed from before that?
She: At XXX hospital, a year before that.
Me: Were you dilated then?
She: No.
Me: Then, when was the last time you got dilated?
She: Don’t remember
I stopped asking her anything further. What I’m trying to highlight here is that in our very hurried lives we forget to take care of one of God’s most precious gifts. Our eyes. Since our lives are tightly bound by the wrist watch that we all wear, it has become difficult to go to an ophthalmologist to get our eyes checked properly. After all who’d want to sit for an hour with uncomfortable dilating drops put into your eye till you are completely unable to see clearly. What’s more annoying is that the effect of the dilating drops last the rest of the day, so that ruins your chances of watching that interesting movie on TV!
Unfortunately, as ophthalmologists, our job is not done by just prescribing your spectacles. We have to look at your eyes outside to inside, and ensure that you are not at risk for any complications of myopia. Most of the complications are related to the difference in the structure of the myopic eye.
The Myopic eye is essentially a ‘stretched’ eye. Which means, the eye is longer from front to back when compared to a normal eye. This mean rays of light have to travel further backwards to fall on the retina. Unfortunately, only the outer layers of the eye stretch; the other structures in between do not stretch or change proportionately. Therefore the crystalline lens fails to bring light entering the eye to a point focus on the retina. This focal point, at which a clear image is obtained falls somewhere in front of the retina.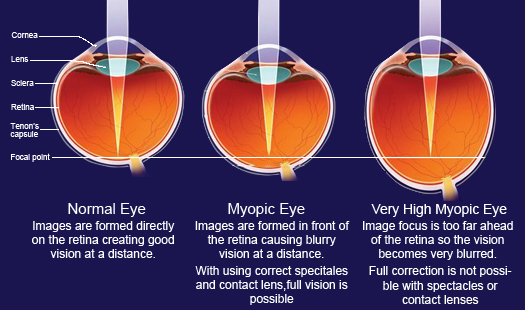
When myopia is mild or moderate good vision can be obtained with corrective spectacles. However, even such eyes can develop some changes in it that can cause severe vision loss. The belief that everything is alright with your eye once your spectacle number stabilizes is wrong. There are changes that take place within the eye, that you may not be able to notice, but which can cause some serious problems with vision.
These changes are related to the stretching of the eyeball due to progression if myopia. Most of the vision threatening changes occur in the far periphery initially. The retina is stretched so much that it starts ‘cracking‘, something similar to old clothes getting frayed after many washes.

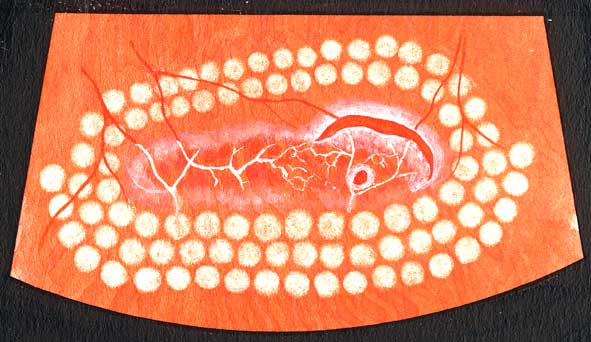
Pic courtesy: Optos
This ‘cracking’ is called lattice degeneration (see above). These cracks can eventually stretch too much to form ‘tears’ or ‘holes’. (see below)
Once a hole or tear appears you might get symptoms of streaks of light flashing past your face. These flashes can be normal too. The next time you feel a sneeze coming up just close your eyes and let go. You’ll see white spots of light flying on the periphery of your vision that will last for a few seconds.
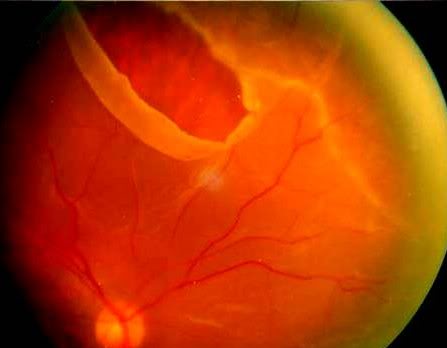
Sometimes, especially in higher degrees of myopia the vitreous (the jelly like substance inside the eye) liquifies and it is this liquified vitreous that appears as small dots or shadows (called floaters) in your vision when you look at a bright background. If this fluid vitreous goes though the tear it can separate the retina from the underlying layers, a condition called retinal detachment. (see below)
There will be a sudden drop in vision with flashes that are continuous. This is an ophthalmic emergency. Unless the retina is surgically replaced immediately there is great risk of permanent loss of vision. Retinal detachment can be prevented to a large extent by using lasers to ‘fence off’ the hole (see below) and prevent the liquid vitreous going under the retina.
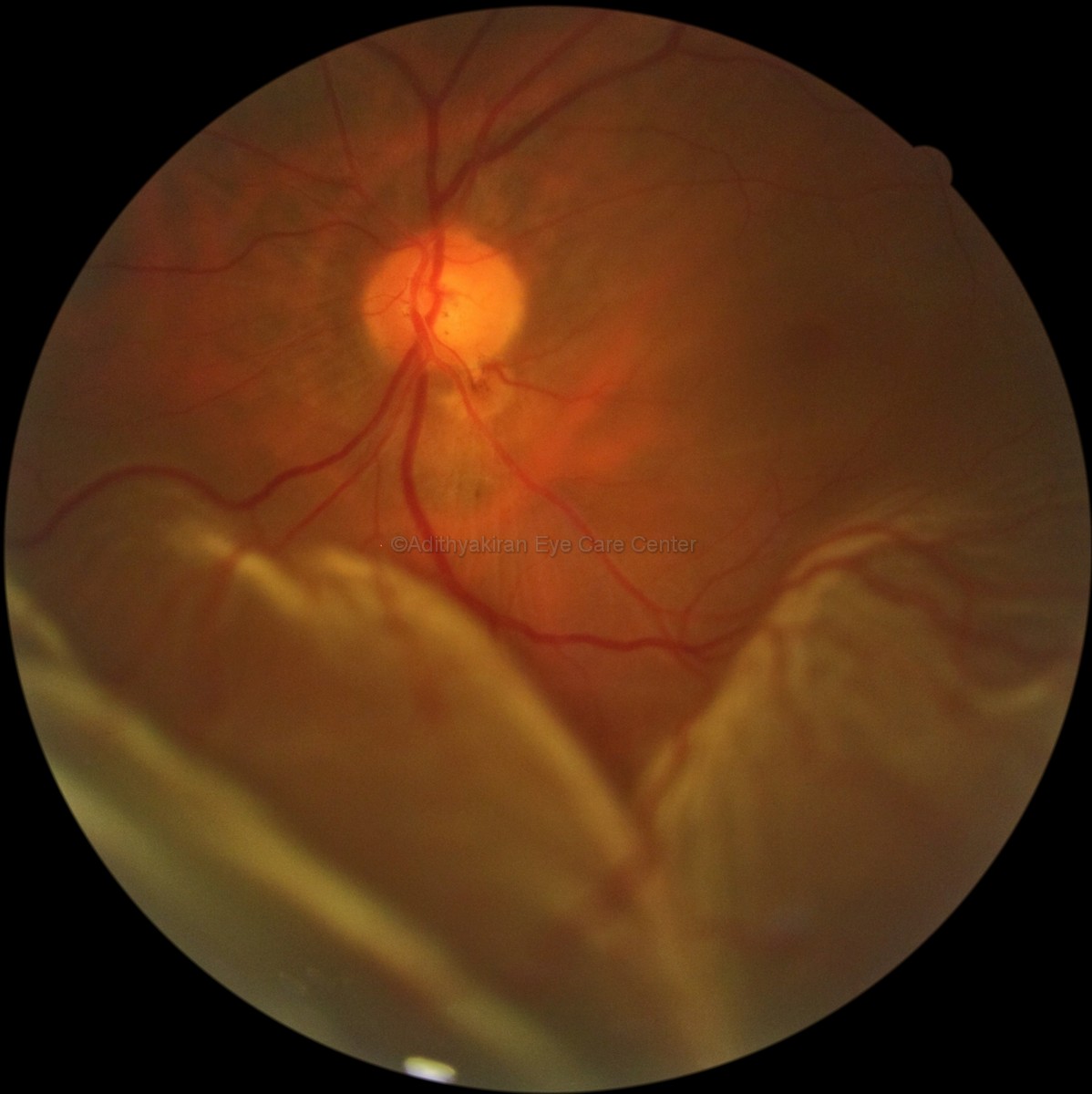
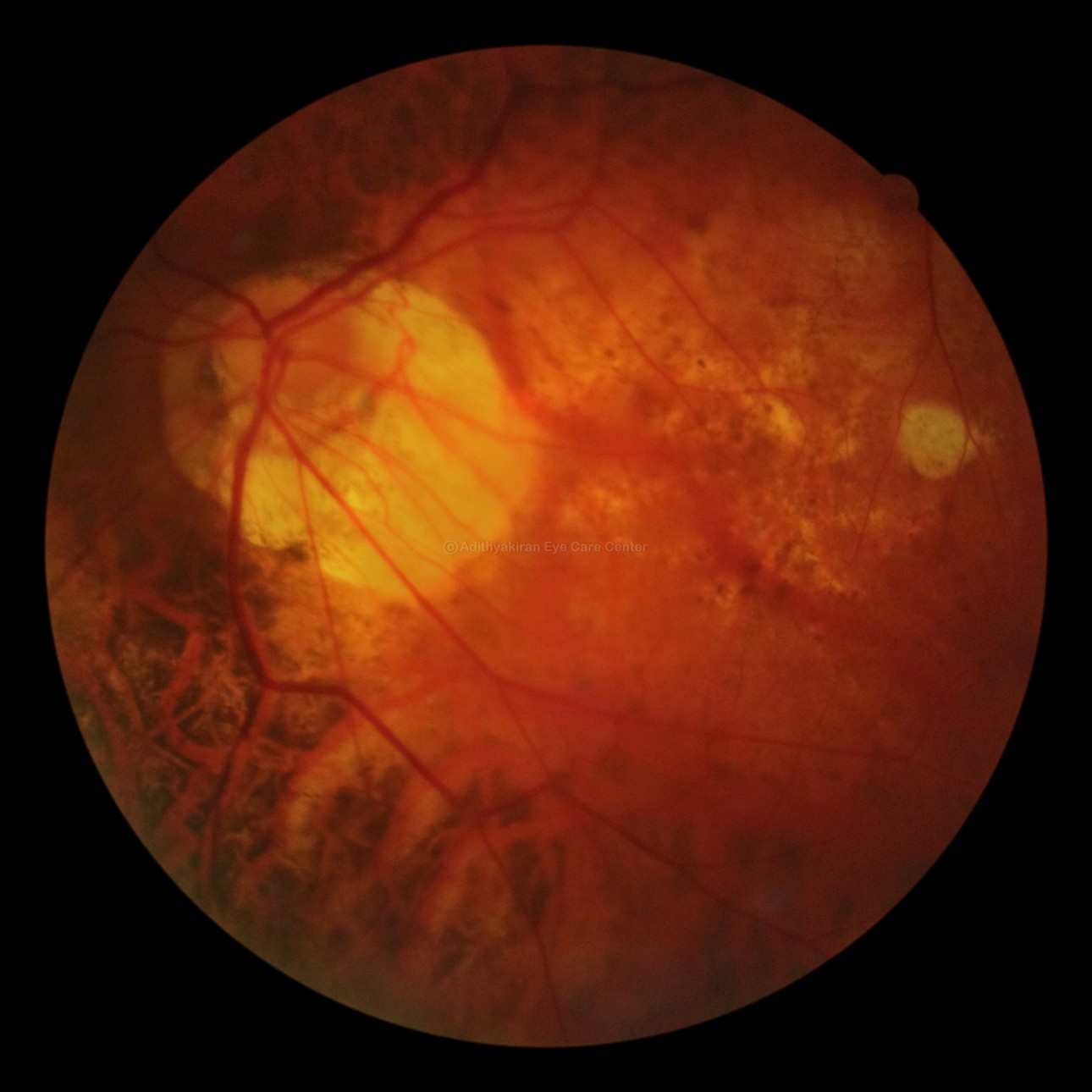
In some advanced cases of myopia the eyeball stretches backwards so much that the retina and underlying structures get thinned and damaged near the optic nerve head and the macula (the part of the eye that controls fine vision). That condition is called a posterior staphyloma and it usually results in poor central vision.

Compare this to a relatively normal fundus in this picture below.The disc and the blood vessels are spread out on a very uniform background retina unlike in the pictures above.

So the next time you go to your ophthalmologist don’t just say, “I’ve come to check my number”; say “I’m here to check my eyes inside and out”.
Make sure you get all these tests done:
- Visual acuity with and without spectacles
- Best Corrected Visual Acuity if your spectacles feel inadequate
- Intraocular pressure
- Retiniscopy
- Ophthalmoscopy, including indirect ophthalmoscopy if you have higher degrees of myopia
EVENING UPDATE 6.30PM
I’m updating here because of a patient who walked in an hour ago. She had undergone LASIK in 2002 and her spectacle number before the procedure was -14 diopters. After LASIK it had reached near about zero and is still stable. If you have undergone LASIK to get rid of your glasses please do keep in mind that this procedure only alters the front of your eyes. All the serious changes occur within the eye and therefore you need to continue getting your eyes checked every year, as described above. Otherwise, subtle progress can be missed and you could end up with a sight threatening complication!





