Corona has locked most of us up inside and along with us are the various addictive gadgets from the cell phones, computers, tablets, and televisions. The new norm is ‘work from home’ and employers are expecting more out of their employees because they are working in their comfortable homes! Some governments and educational institutions in their wisdom have also joined together to get students to also ‘work from home’ through unscientific online classes. I know of a school that has online classes for four hours a day, in two sessions of two continuous hours of lessons! What they don’t realize is that both the students and teachers are not tuned to such a sudden shift in the method of teaching.
To all of us, if not most of us, a classroom is a place where there is a one to one interaction between student and teacher. Most teachers are used to a room full of noisy, happy students whom they continuously monitor as a group. For the students, spending a day in school with their friends, sharing their lunches and playing together is a part of growing up and staying healthy. Unfortunately, the fear of Covid – 19 and the lockdown has turned the world upside down. The system of online classes, especially for school students here, is a stressful experience for not only the teacher and students but also for the parents and guardians of the child because the students are expected to be monitored during such online classes by a family member!
When you put a small child in front of a computer or a digital device there are certain health issues that we must take into consideration. It could be related to the device itself or the improper use of it. If you have a child attending online classes, keep the following things in mind.
The Device and its surroundings
Online classes are being conducted on either a computer, a mobile phone or tablet PC. Remember none of these gadgets can a substitute for a book. Neither can a keyboard, especially touch screen keypads, replace the pen and pencil.
Between the computer and the cell phone or tablet, the former is a better option because the screen is bigger. A page from a book can be read more comfortably on a computer than with a phone or tablet. A normal A4 sized page can be viewed in the normal size on a larger computer monitor and may only require the page to be moved up and down. On a tablet or mobile screen you have to enlarge the page to see in a sufficiently large font size but then only a very small portion of the page can be viewed at any time and it will have to be scrolled in four different directions.
The computer can be kept on a table and viewed from a proper distance, but the smaller devices have to be handheld and so are too close to the eyes. If the online classes are going to be a long term and regular affair, it is better to get a desktop computer. These days basic computers are less expensive then mobile phones anyway! If not a tablet PC with a large screen is a possible option.
Most of these devices are designed with an adult in mind so setting up the computer for a child should be different. Normally, the screen should be positioned in such a way that we don’t have to bend our necks to look at it. It should be placed about two feet away and at a level where you only have to move your eyes slightly lower, about 15 to 20 degrees downward, to see the screen comfortably. For a child, you may have to make them sit on a higher chair so that the same angle of view is achieved. Similarly, the mouse and keyboard may also have to be repositioned to suit the child. The feet of very small children will not reach the floor while sitting on a regular chair, so a foot support would be a good idea. Alternatively, a table and chair that are lower and suits their height, could be a possible option.
All computers and digital devices are self-illuminated. Therefore, the ambient light in the room where it is used should neither be very dim nor too bright. The screen brightness should be adjusted to a level that is comfortable for the child and doesn’t make the child squeeze the eyes. Similarly, ensure that, especially if the device is near a window or light source, that the external light doesn’t hit the screen to cause uncomfortable glare.
Problems with excessive use of digital devices and computers
- Posture related problems. Most children using mobile devices are used to holding them close. They either sit hunched over it or lie stretched in an odd posture on a bed or settee. This can result in muscular aches, back and shoulder It is easier to control posture with a correctly adjusted desktop computer but with laptops or mobile devices it will require repeated reminders to maintain a healthy posture.
- Wrist pain. All keyboards and mice are designed for an adult so a very small child might find it very difficult to hold and manipulate the mouse or type comfortably. Excessive forcible twisting movements of the wrist can cause pain and eventually lead to a condition called carpal tunnel syndrome.
- Eye strain. Children cannot recognise the problems they experience while using these devices and will continue using them if they are performing and ‘enjoyable task’ like gaming. It is the responsibility of the elders to ensure that prolonged use should be curtailed with intermittent breaks. Otherwise, the children can end up with any of the following:
- Dry eyes due to staring unblinkingly at the screen for hours
- Focussing problem because of continuously looking at a fixed distance. The eyes have to be maintaining focus at a closer distance and the child eventually has ‘accommodative spasm’.
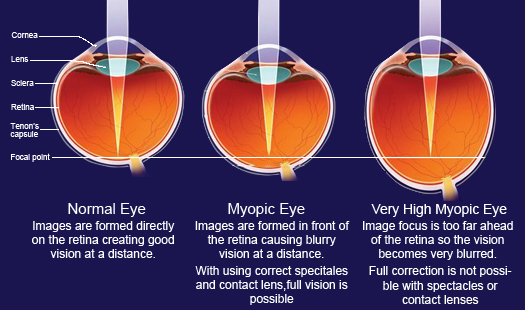
- Development of myopia (short sight) is common because the eye is always focussing at near objects and wont refocus for distance. In addition, not spending enough time outdoors can also contribute to progression on myopia.
- Children using these devices get fatigued easily because they are constantly sitting in one place and in an posture that doesn’t let the joints and muscles relax.
- A good night’s rest is essential for healthy life. Digital devices can affect sleep because of the ‘blue light’ effect if the child uses the device late at night.
- Children addicted to digital devices will show little interest in physical activity and that can cause obesity with its attendant risks.
Scheduling online classes appropriately
From the interaction I’ve had with the children, their parents and a few teachers, I feel there is something fundamentally wrong in the approach of the school authorities, politicians and other officials concerned with education. They seem to be in a hurry to make up for lost time and also ensure that running a school is a viable proposition in the middle of the this Covid crisis for which there is no end in sight.
Before planning classes we should look at how attentive a child will be in a monotonous environment.
A simple way of calculating the attention span of children according to child development experts is to multiply the age with a factor of two or three, (may differ depending on the source of information). This gives the number of minutes a child can pay constant attention to the task at hand. So if we calculate for the ages two to sixteen these are the approximate figures.
|
AGE IN YEARS |
ATTENTION SPAN IN MINUTES | AVERAGE ATTENTION SPAN |
|
2 |
4 to 6 | 5 |
|
4 |
8 to 12 |
10 |
|
6 |
12 to 18 | 15 |
| 8 | 16 to 24 |
20 |
|
10 |
20 to 30 | 25 |
| 12 | 24 to 36 |
30 |
| 14 | 28 to 42 |
35 |
| 16 | 32 to 48 |
40 |
You can see that, younger the child, lesser the attention span. This calculation may be alright for a school in its proper environment, a classroom, but when it comes to online classes the arithmetic must change. In a classroom, there are classmates, friends and teachers interacting constantly on a personal level. To most children being in a noisy classroom is far more fun than interacting on an impersonal level with a device. The comforting touch of the teacher when things look down, exchanging childhood mischief with friends and sharing lunches are all missing! Instead, the child is forced to sit and concentrate at the job at hand, often with an elder supervising, in a rather stifling environment.
From the parent’s perspective, especially if they are both working, it is an exceedingly difficult proposition to manage this new system of online classes. Either one of them will have to take leave to remain with the child at home during these sessions. In case there are grandparents around, they could be the backup team but, in our environment, especially in poorer families they may not be tech savvy or educated enough to interact with the teachers on behalf of the children.
The problem does not end there. The teachers are also a suffering lot. One teacher told me that in the school she taught, the classes were conducted in two sessions. From 9 am to 1.30 pm for higher classes then from 4 pm to 7.30 pm for the smaller children. They would have a short break each hour but the difficulty was getting all the students back for the next round. They would have wandered off and will have excuses like internet issues and power failures to explain their absences! Not only that, the teachers would have time to prepare for the next day’s classes only after the day’s were over. Which means they would be up working till midnight and beyond!
We should take into consideration that even the teachers are probably more trained towards a classroom environment where they interact directly with their students. Therefore, when you are suddenly thrown into a situation where you are forced to learn and do something new and completely out of your comfort zone, problems are bound to crop up. 2020 as a year is going to continue in fits and jerks and we have to take each day as it comes. It is impossible to plan for more than a few days ahead as the behaviour of the pandemic is unpredictable. This year, not only for academics but everything else, will be a washout and therefore putting undue pressure on students and their teachers might backfire.
It is also a time where the parents will have to brush up on their digital skills or learn it from scratch. Online classes will be the norm for a few more months, perhaps longer, and only time will tell how beneficial it is to promoting education. Meanwhile, it would be better if parents, teachers and school managements are prepared properly for this unforeseen and unavoidable situation we are in.
Tips for managing an online class
- Set up the hardware in a properly lit room without any other distractions like televisions, refrigerators or snack cupboards. Children’s attention can easily be diverted.
- Make sure that the child is seated comfortably otherwise they will get restless and attention will wander.
- If an adult supervisor is in the room with the child, it is better they avoid fiddling with their cell phones or other gadgets. A newspaper or book is a better option.
- If there are other people in the house, ensure that they don’t disturb during the sessions. If they are watching TV (best avoided), listening to music or plain gossiping, keep the volume to the absolute minimum.
- Sitting in front of a digital device or computer forces the eyes to continue focussing at a very close distance, unlike in a classroom where the eye muscles can relax as the sight swings from the board to the desk and elsewhere. It means that the eyes become stressed faster so online classes should never run continuously for more than 20 minutes for small children or 30 minutes for bigger children.
- Remember the 20-20-20 rule. Continuous working on a self-illuminated screen at close distance can be tiresome, especially for a child. Therefore, after every 20 minutes (or 30 for older children) ask the child to look at some object 20 feet away for 20 seconds. That way, they eyes will be able to loosen up to relieve the strain of focusing continuously at the screen.
- Ask the child to blink frequently so that the tear film resurfacing can prevent drying up of the eyes. They will have to be reminded frequently till it becomes second nature to them.
- A break of 5 minutes should be given between classes, which will allow the child to relax focus and loosen up limbs and the body. If the teacher or parent can make the child do some simple loosening up exercise during the breaks, it would add to the excitement.
- Allow the child to take a few sips of water or juice in between. Snacks can be reserved for the longer breaks.
- It is better to confine the child to the room and not allow him or her to leave the immediate ‘classroom’ environment. Otherwise, they may lose the concentration. Let them learn to see the ‘virtual classroom’ like a real one and behave accordingly.
These are random thoughts that occurred to me as I’m seeing increasing numbers of children presenting with various complaints after the online classes have started. Please get in touch with me for any other doubts or clarification you may require.
Dr. Rajesh Radhakrishnan